An understanding of when the daily infection is at its peak in relation to the concept of the flattening of the curve on the spread of Covid-19 will throw some lights on what wave of the pandemic we are at, and what are to be done in facing the current fourth wave of infections.
Flattening of the infection curve means reducing the number of infections by influencing its transmission rate via controlling the virus reproduction rate (R nought) through preventative measures of reducing social contacts such as the movement control order (MCO), and at the same time upgrading the capacity of the healthcare system to cope with an increasing number of infections.
The result – the number of infections will peak slowly and lower as shown by the blue flattened curve in the diagram below with relatively fewer cases compared to a scenario without any intervention (red curve) at all.
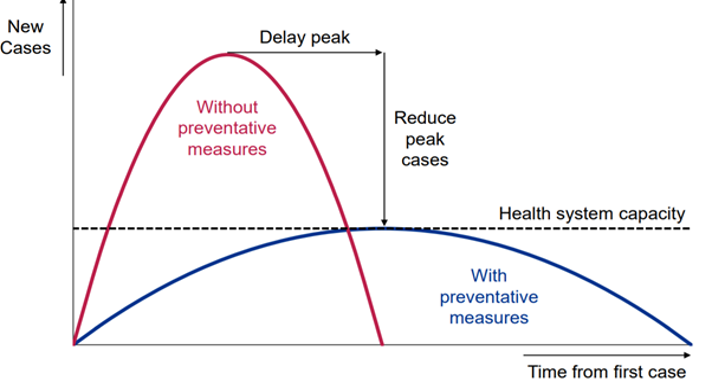
What the graph is telling us is, there are two phases of the flattening of the curve. The first phase of flattening of the curve occurs when the daily infection figure reaches its peak. At this stage the curve will plateau (flatten). The curve cannot flatten for as long as the peak is not reached.
When the observance of the MCO “culture” which indicates social responsibility of the rakyat is in action and becomes the salient feature of the MCO – such as observing social/physical distancing, practising regularly personal hygiene like washing hands, avoiding large gathering and wearing a mask in public – a second phase of flattening of the curve to its floor as shown in the diagram, which will then taper to a zero infection will occur.
In Malaysia, the first wave of the Covid-19 pandemic last year began from Jan 25 to March 2. On Jan 25, Malaysia announced its first three cases of Covid-19. The peak daily infection for this first wave was recorded on Feb 8 with four cases. The infection curve started to flatten to its floor with zero cases for 11 consecutive days beginning Feb 16, indicating the ending of the first wave.
On Feb 27, these zero cases came to an end but because the new cases from that day until March 2 did not breach the peak of four cases, at this stage it was still the first wave.
The second wave began on March 3 with seven cases, breaching the peak of the first wave (4), and ended on Oct 1 (260 new cases). Soon after the daily infection recorded a three-digit figure for the first time ever on March 15 with 190 cases, MCO 1.0 was announced by the government, effective from March 18.
The peak for this second wave was recorded at 277 cases on June 4. Since then, the curve has flattened, with new daily cases thereafter going up and down like a yoyo where there are instances of a one-digit daily infection for some days. But when it went up, it never breached the peak of 277 cases. This second wave never witnessed the second phase of the flattening of the curve to its floor (zero cases).
On Oct 2, the third wave began with new cases at 287, breaching the peak of the second wave (277). The peak of the third wave was 5,728 new cases recorded on Jan 30 this year. The third wave ended on May 18 with 4,865 new cases without flattening of the curve to its floor (zero cases), as in the second wave.
On May 19, we saw new cases at 6,075, breaching the peak of the third wave and signalling the start of the fourth wave. Has the fourth wave reached its peak? The dicey thing about determining the peak is, it is only known in hindsight.
When the peak of the second wave was recorded at 277 cases on June 4 or the peak of the third wave on Jan 30 (5,728), no one knows on that day that this number was going to be the peak.
But having a rough idea of when the peak will be reached is important because it gives us a clue to the flattening of the infection curve or at least give us a sense of relief that the worst is over (without any implication that we are out of the woods).
Today (June 1) we are on the 14th day of the fourth wave. So far, the highest daily infection recorded within these 14 days is 9,020 cases on May 29. Could this be the peak especially after a drastic drop in the next two days of 6,999 (May 30) and 6,824 yesterday (May 31)? Hopefully so, although we can’t be certain.
However, from studying the pattern of the previous waves, we know that the peak in the first wave was reached 14 days after Covid-19 made its appearance in this country; the peak of the second and third waves were both reached three months after each wave began. In term of duration, the first wave lasted for one month and six days; the second wave, seven months; and the third wave, seven months and 16 days.
This tallies with science which says subsequent waves will be more lethal, infectious and take relatively longer time to end because of the various mutations of the virus which lead to the emergence of various tough variants.
But what is of concern here is that even if preventative measures in the MCO are there, the path to a flattening of the curve will be longer if the capacity of the healthcare system is not upgraded.
With intervention in the form of an urgent upgrading of the capacity of the healthcare system, more ICU wards, more quarantine spaces, more ventilators, more equipment for testing and screening, and more protective gear for the frontline doctors and nurses can be provided, which in turn will ensure the number of infected people getting the needed medical attention will increase, thereby increasing the recovery rate and reducing the fatality rate, all these under a scenario of a 2% case fatality rate, ceteris paribus – everything else remain constant.
This in turn will give some breather for “regrouping” by allowing some frontline doctors and nurses to rest, reducing further the number of infections among healthcare workers at the frontline.
A proviso though: unlike in economic theory, in real life ceteris is not paribus and in the absence of other preventative measures, like the implementation of the current Full MCO (FMCO), this breather, which is a narrow window of opportunity, will deteriorate soon enough because it is also a breather for the remaining Covid-19 virus to buy time and fortify themselves via more mutations for another wave of attack.
Judging by Prime Minister Muhyiddin Yassin’s speech yesterday when he unveiled a RM 40 billion Pemerkasa Plus in economic aid, which includes RM 5 billion direct fiscal injection from the federal government where quite a huge chunk of it went to the Health Ministry for upgrading the capacity of the healthcare system, he is indeed moving in the right direction, making Malaysia a good model for countries which were late in taking such action because of bureaucratic paralysis.
Among the action taken to boost public healthcare capacity:
- RM 450 million to increase hospital beds and procure equipment for intensive care units, including at teaching hospitals of public universities at military field hospitals;
- RM 550 million for spending related to Covid-19 including increased operating and management expenses, procurement of medicines and reagents, and appointment of contract officers; and
- Extend the service of 14,000 contract medical officers and nurses until 2022 and appoint 500 healthcare workers who are due for mandatory retirement this year on a contract basis.
Hopefully, the brief respite afforded to us due to these preventative actions of an FMCO and the upgrading of the healthcare system can extend a little bit further the respite by shortening the time taken for the curve to reach its peak and also the duration of the fourth wave.
But the saving grace to all this is the vaccination programme being carried out now that will just speed up the discovery process of the peak and shorten the duration of the current wave via herd immunity. Also, who knows during this respite, an important approved drugs that can cure Covid-19 will emerge, which will further flatten the curve to the floor.
And here’s where the government needs your help. Whether you are in the frontlines of the battle – healthcare and essential services manpower – or behind the lines, each one of us have a duty to perform: those at the frontlines are working for the sake of those staying at home during FMCO, and those behind the lines must stay at home as much as possible during the FMCO for the sake of those working at the frontlines.
Jamari Mohtar is Director, Media & Communications at EMIR Research, a think tank focused on strategic policy recommendations based on rigorous research.
[This article belongs to The Malaysian Medical Gazette. Any republication (online or offline) without written permission from The Malaysian Medical Gazette is prohibited.]