Introduction

Quietly yet persistently, obesity has emerged as one of the most profound threats to women’s reproductive health in the twenty-first century. The rising prevalence of obesity among women of reproductive age has transformed fertility from a purely reproductive concern into a complex metabolic and molecular challenge. For many women, the journey toward conception becomes longer, more uncertain, and emotionally taxing when excess adiposity disrupts the finely tuned biological systems that govern reproduction.
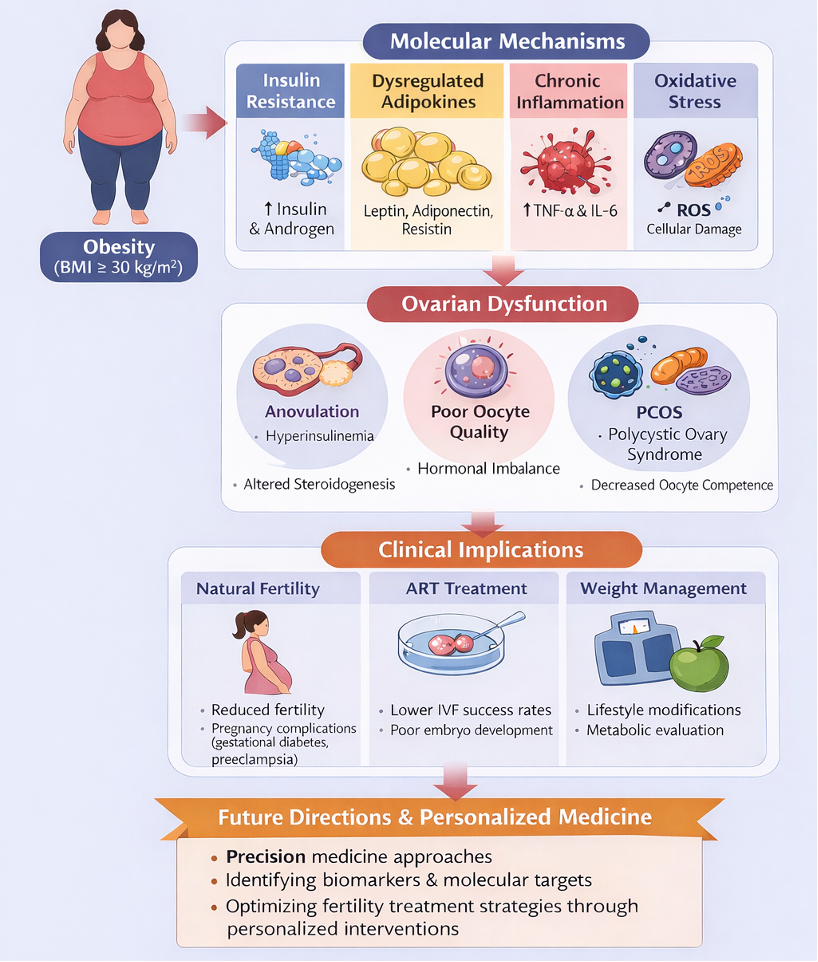
Female fertility relies on an intricate interplay between endocrine regulation, metabolic homeostasis, and molecular and cellular signalling. The hypothalamic–pituitary–ovarian (HPO) axis functions as a precisely coordinated biological orchestra, in which hormonal cues and intracellular pathways must operate in synchrony to ensure ovulation, fertilization, and embryo implantation. Obesity profoundly disturbs this equilibrium. It interferes with ovulatory function, compromises oocyte and embryo quality, and reduces the success of fertility treatments. Moreover, obesity is closely linked to polycystic ovary syndrome (PCOS) and other metabolic disorders through dysregulated hormonal signalling, further amplifying reproductive dysfunction.
In this context, a translational approach is imperative. Bridging molecular discoveries with clinical practice and preventive strategies is essential to address obesity-related infertility effectively. Identifying key proteins, genes, and signalling pathways involved in reproductive dysfunction offers new opportunities for precision diagnostics and personalized fertility care.
Obesity
Clinically, obesity is defined as a body mass index (BMI) ≥ 30 kg/m². While this definition is straightforward, its implications for female reproductive health are far-reaching. Globally, obesity rates among women of reproductive age continue to rise, with particularly rapid increases observed in middle-income countries undergoing nutritional and lifestyle transitions.
Malaysia exemplifies this epidemiological shift. Rapid urbanization, increased consumption of energy-dense diets, and sedentary lifestyles have contributed to a growing burden of obesity among young women. Socioeconomic and environmental determinants further compound this issue, positioning obesity as a multifactorial public health challenge rather than a purely individual condition.
From a reproductive perspective, obesity is associated with higher rates of subfertility and infertility, placing increasing strain on reproductive health services. These trends underscore the urgent need for integrated strategies that address both metabolic health and fertility outcomes.
Insulin Resistance
Insulin resistance represents a central metabolic disturbance in obesity. Excess adiposity promotes peripheral insulin resistance, leading to compensatory hyperinsulinemia. Elevated insulin levels exert direct effects on the ovary, stimulating androgen production and disrupting steroidogenesis.
This hormonal imbalance interferes with gonadotropin signalling, particularly follicle-stimulating hormone (FSH) and luteinizing hormone (LH), thereby impairing follicular maturation and ovulation. Clinically, these disturbances manifest as anovulation, irregular menstrual cycles, and reduced fertility. The strong association between insulin resistance and PCOS further highlights the pivotal role of metabolic dysregulation in female reproductive disorders.
The Role of Adipokines
Adipose tissue is now recognized as an active endocrine organ that secretes a wide range of bioactive molecules known as adipokines. Among these, leptin, adiponectin, and resistin play critical roles in linking energy balance to reproductive function.
In obesity, leptin resistance develops despite elevated circulating leptin levels, leading to impaired energy-sensing signals essential for normal reproductive regulation. Concurrently, reduced adiponectin levels diminish insulin sensitivity and anti-inflammatory protection, while increased resistin exacerbates insulin resistance. Collectively, these alterations disrupt HPO axis signalling and compromise reproductive competence.
Chronic Low-Grade Inflammation
Obesity is characterized by a state of chronic low-grade systemic inflammation. Increased secretion of pro-inflammatory cytokines, including tumour necrosis factor-α (TNF-α) and interleukin-6 (IL-6), extends beyond metabolic tissues and directly affects ovarian function.
At the molecular level, sustained inflammation alters gene expression in granulosa and cumulus cells, which are essential for supporting oocyte maturation. Disruption of the follicular microenvironment results in reduced oocyte quality, impaired embryo development, and compromised implantation potential.
Oxidative Stress
Another critical consequence of obesity is the imbalance between reactive oxygen species (ROS) production and antioxidant defence mechanisms. Excessive oxidative stress induces DNA damage and mitochondrial dysfunction within oocytes, undermining cellular energy supply and developmental competence.These molecular insults adversely affect early embryonic development and are associated with an increased risk of early pregnancy loss, further diminishing reproductive success in obese women.
Effects of Obesity on Ovarian Function
Ovulatory dysfunction is a hallmark of obesity-related reproductive impairment, manifesting as anovulation or oligo-ovulation. Beyond ovulatory defects, obesity negatively influences oocyte quality through reduced oocyte competence and altered expression of key genes such as GREM1, PTGS2, and BMP15. These genes are critical mediators of communication between the oocyte and surrounding cumulus cells, a process essential for optimal oocyte maturation.
In women with PCOS, obesity acts as a potent aggravating factor. Excess adipose tissue and insulin resistance intensify hyperandrogenism, while alterations in the FSH:LH ratio contribute to menstrual irregularities and further disruption of ovulatory function.
Clinical Implications
Obese women often experience prolonged time to conception and face higher risks of obstetric complications, including gestational diabetes, preeclampsia, labour complications, and macrosomia. These risks emphasize the importance of preconception counselling and early weight management strategies incorporating nutritional optimization and physical activity.
In assisted reproductive treatments such as in vitro fertilization (IVF) and intrauterine insemination (IUI), obesity is associated with diminished ovarian responsiveness, higher gonadotropin requirements, and lower implantation rates. Embryo quality is frequently compromised by an unfavourable metabolic milieu. Consequently, assessment of BMI and metabolic status prior to Assisted Reproductive Technology (ART), along with meticulous antenatal care, is essential to optimize outcomes.
Clinical Management Strategies
Management of obesity-related infertility focus on lifestyle modification, including dietary intervention and regular physical activity. Even modest weight loss can significantly reduce insulin resistance, restore hormonal cyclicity, re-establish ovulation, and improve pregnancy rates.
In selected cases, pharmacological interventions such as appetite suppressants or insulin-sensitizing agents like metformin may be employed. Bariatric surgery represents an option for severe obesity, although its reproductive implications require careful multidisciplinary evaluation.
Education and Awareness
Raising awareness of the relationship between obesity and fertility is crucial for medical students, healthcare professionals, and the broader community, particularly younger populations. Framing obesity as a reproductive health issue rather than solely a metabolic disorder reinforces the importance of early prevention. A holistic educational approach that integrates biological, clinical, psychological, and lifestyle perspectives is essential for sustainable behavioural change.
Future Directions and Personalized Medicine
Advances in molecular biology, genomics, and omics technologies are reshaping the future of fertility care for obese women. Deeper insights into genetic variability, gene expression profiles, and proteomic and metabolomic signatures offer unprecedented opportunities to identify molecular biomarkers predictive of subfertility, treatment response, and pregnancy outcomes.
Personalized medicine in female fertility may incorporate individualized metabolic and hormonal profiling, molecular analysis of granulosa and cumulus cells, and characterization of obesity-disrupted signalling pathways. Variations in genes involved in insulin signalling, adipokine regulation, and inflammatory responses may enable stratification of patients into biologically distinct subgroups, guiding targeted lifestyle interventions, pharmacotherapy, or optimized ART protocols.
Integration of molecular data with clinical parameters through bioinformatics and artificial intelligence holds promise for improving predictive accuracy and clinical decision-making. Such approaches may reduce ineffective treatments and alleviate the physical, emotional, and financial burdens associated with infertility care.
Nevertheless, translation of these innovations into routine clinical practice requires robust translational research and multidisciplinary collaboration among molecular scientists, reproductive clinicians, nutritionists, and data scientists. In the long term, personalized fertility care has the potential not only to enhance treatment success but also to support early prevention and long-term reproductive health preservation.
Conclusion
Obesity exerts multifaceted effects on female fertility through interconnected molecular, metabolic, and inflammatory pathways. These disruptions compromise ovarian function, reduce the success of assisted reproductive technologies, and adversely affect pregnancy outcomes. Addressing obesity-related infertility demands an integrated molecular–clinical framework supported by continued translational research, personalized interventions, and early preventive strategies to safeguard women’s reproductive health.