 Established as one of the world’s earliest pioneers of medicine, Egypt houses everything we know from ancient inventions such as mummifications in the desert to methods of simple non-invasive surgeries. Although it is poorly understood, it served as the spark that lit the trail to of medical advancements we see these days. Previously, development of theories were pretty much simplistic. The knowledge of blood circulation was likened to the River Nile as a channel that conveys water and nutrition to the crops; if it is clogged, the water supply would not be able to reach the crops and consequently became unhealthy. It was this basic physiology that begets several other theories and assimilated into understanding the endless complexities of the human body.
Established as one of the world’s earliest pioneers of medicine, Egypt houses everything we know from ancient inventions such as mummifications in the desert to methods of simple non-invasive surgeries. Although it is poorly understood, it served as the spark that lit the trail to of medical advancements we see these days. Previously, development of theories were pretty much simplistic. The knowledge of blood circulation was likened to the River Nile as a channel that conveys water and nutrition to the crops; if it is clogged, the water supply would not be able to reach the crops and consequently became unhealthy. It was this basic physiology that begets several other theories and assimilated into understanding the endless complexities of the human body.
Cataract eye surgery first began in Egypt. It all started when the Pharaoh complained that he could no longer see his Pyramids and ordered a doctor to operate on him. The Egyptian special surgeon to the Pharaoh would chew on an opiate concoction, an ancient anaesthetic preparation and spit it into the eyes of his patient before conducting the surgery. Emerged from this idea, was induction of anesthesia through inhalation and intravenous route. Several pharmacopeia written on papyrus also provided evidence on the existence of gynaecology, obstetrics, surgery and pharmacology several thousands years before they were better studied. It is a fact that western inventions took a leaf out of the pages of the Egyptians before developing their own ideas.
Source: www.cab.unimelb.edu.au
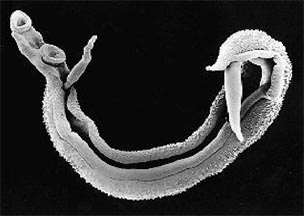
Ancient intricacies and wonders do not just stop there. Egypt is also famous for many diseases. Bilharzia or Schistosomiasis, is a disease caused by parasites namely Schistosoma mansoni, Schistosoma haematobium and Schistosoma japonicum. It has a long trail of history here and it was first described by Theodore Maximillian Bilharz, a German physician working in Kasr-El-Ain Hospital in Cairo who unfortunately died from another famous disease in Egypt which is Typhus, a bacterial disease. The government spent sixty years trying to curb the disease and have only recently seen positive results. Bilharzia is harvested in snails and not found within the vicinities of Cairo because of the absence of water canals but continues to dwell in the rural area where the water canal maintenance is poor. It also contributes to the rise in the incidence of urinary bladder cancer and liver diseases in Egypt, complications of the disease which has not yet been fully eradicated.
 Although immunisation coverage has been doing quite well in Egypt, several preventable diseases like Diphteria, a deadly bacterial disease, can still be contracted particularly in rural areas covering the lesser population who do not comply to the vaccines. One of my lecturers has encountered a patient with Diphteria previously. The patient presented with extreme weakness when he arrived at the hospital where my lecturer worked as a junior doctor. However, his fever was low. He had increased heart beat not proportionate to the fever and a large neck swelling appearing like a Bull’s neck because of the high level of toxins in his blood. My lecturer came to a swift diagnosis although the disease is often identified by exclusion as it is rare and patient should have been vaccinated and protected. He injected several doses of anti toxins before the laboratory results suggested that it was positive and the patient was eventually saved from the fatal disease.
Although immunisation coverage has been doing quite well in Egypt, several preventable diseases like Diphteria, a deadly bacterial disease, can still be contracted particularly in rural areas covering the lesser population who do not comply to the vaccines. One of my lecturers has encountered a patient with Diphteria previously. The patient presented with extreme weakness when he arrived at the hospital where my lecturer worked as a junior doctor. However, his fever was low. He had increased heart beat not proportionate to the fever and a large neck swelling appearing like a Bull’s neck because of the high level of toxins in his blood. My lecturer came to a swift diagnosis although the disease is often identified by exclusion as it is rare and patient should have been vaccinated and protected. He injected several doses of anti toxins before the laboratory results suggested that it was positive and the patient was eventually saved from the fatal disease.
 The healthcare sector in Egypt probably bears the brunt of the challenges. The health staff have to overcome the disease stigmatization among the closed and conservative Egyptians. This also includes funds and equipment shortage in government hospitals. Some vital departments like paediatrics do not have defibrillator, a device used to correct abnormal heart beat, thereby causing some potentially salvageable diseases to end in death. Some diagnosis were made based on clinical findings only because some laboratory tests would require hundreds of pounds which is too much for the poor. The clinicians usually opt for the cheaper alternatives which of course offers a lower sensitivity and specificity results and may lead to a misdiagnosis. A cardiologist could diagnose heart disorders perfectly by using only a Chinese-made-stethoscope worth a few pounds. That is typically how wisdom runs in the blood of every devoted doctor working in Egypt.
The healthcare sector in Egypt probably bears the brunt of the challenges. The health staff have to overcome the disease stigmatization among the closed and conservative Egyptians. This also includes funds and equipment shortage in government hospitals. Some vital departments like paediatrics do not have defibrillator, a device used to correct abnormal heart beat, thereby causing some potentially salvageable diseases to end in death. Some diagnosis were made based on clinical findings only because some laboratory tests would require hundreds of pounds which is too much for the poor. The clinicians usually opt for the cheaper alternatives which of course offers a lower sensitivity and specificity results and may lead to a misdiagnosis. A cardiologist could diagnose heart disorders perfectly by using only a Chinese-made-stethoscope worth a few pounds. That is typically how wisdom runs in the blood of every devoted doctor working in Egypt.
If you have not visited this country, you might not know how deeply populous the country is. Harbouring approximately eighty-one millions of citizens, hygienic problem comes hand in hand with the progression of most infectious diseases in Egypt. Most Egyptians of low social class are Typhoid disease carrier. Typhoid is basically a bacterial disease transmitted to human through sewage-contaminated food. Thus, one must perfom good aseptic handwashing before eating especially after making contact with them. Rural areas are burdened with a wide array of diseases and sometimes diagnosis takes into account the residence of the patients. For instance, Sharkia and Menoufiya districts are famous for Rhinoscleroma, Nile Delta and Upper Egypt for Bilharzia and many more. The diseases also have a seasonal pattern of transmission. We have no dengue around here but West Nile fever, a disease which also transmitted by mosquitoe, is observed more in late summer or early fall in Egypt.
 We probably knew that the prevalence of Hepatitis C in Malaysia is fairly high. Egypt actually surpasses Malaysia by championing the world’s highest prevalence of Hepatitis C infection. Added to that, the prevalence of Hepatitis B is also worrying. In spite of a shift in the diseases causing death from infectious to non-infectious diseases, infectious diseases are still responsible for considerable part of non-infectious diseases here. For instance, patients suffering from infectious diseases like Hepatitis B and C often get subsequent liver diseases which may end in liver cancer, thus causing double burden on such patients. Lack of needle sterilisation plays a vital role in its dissemination here. However, many brilliant prevention and intervention programmes are designed to reduce the financial and societal cost of this escalating type of cancer in Egypt. When I was in ENT posting, I saw patients with cholesteatoma (a destructive disease inside the ear) almost once a week. The disease has become rare in many parts of the world but still remains a norm here. I also learned that most Egyptians have had their tonsils removed before which pretty much reflects the state of hygiene here as compared to Malaysia.
We probably knew that the prevalence of Hepatitis C in Malaysia is fairly high. Egypt actually surpasses Malaysia by championing the world’s highest prevalence of Hepatitis C infection. Added to that, the prevalence of Hepatitis B is also worrying. In spite of a shift in the diseases causing death from infectious to non-infectious diseases, infectious diseases are still responsible for considerable part of non-infectious diseases here. For instance, patients suffering from infectious diseases like Hepatitis B and C often get subsequent liver diseases which may end in liver cancer, thus causing double burden on such patients. Lack of needle sterilisation plays a vital role in its dissemination here. However, many brilliant prevention and intervention programmes are designed to reduce the financial and societal cost of this escalating type of cancer in Egypt. When I was in ENT posting, I saw patients with cholesteatoma (a destructive disease inside the ear) almost once a week. The disease has become rare in many parts of the world but still remains a norm here. I also learned that most Egyptians have had their tonsils removed before which pretty much reflects the state of hygiene here as compared to Malaysia.
Learning in different clinical and social settings has improved my understanding of diseases and people. Egypt is not only home to the greatest ancient civilization but it is also cited as the locus of many diseases; from rarest to the most common. I am glad that I have worked around the lowest strata of the society with the best clinicians who remain humble and compassionate towards human beings; regardless of the social status. Having spent four years embracing calamities and difficulties I cultivated patience, perseverance, humility and the strong will to fight the everyday odds that stretch beyond my limitations. I witness the desperation of human lives fighting for medications. This teaches me every essence of life and most importantly, on being human. Despite the ongoing unrest, I still admire Egypt at what it has at its best; holistic knowledge.
Ameerul Aiman is a 5th year medical student in Ain Shams University of Cairo, Egypt. Know more about him under the Young Columnists tab.
References:
Interesting on the incidence of cholesteatotoma in your ENT posting. We do encounter similar cases in Sabah but maybe half or 1/3 the number of such cases. Seeing cases greatly improves my learning as compared to just reading in from books. Hope to read more articles from you all.
Thank you for the comment, Dr Ahmad. I’m inspired to be an ENT surgeon like you. Will take the chance to learn everything here 🙂
Thanks for the kind words. Will roll out the red carpet once in the fraternity 🙂
Hi, I am diagnosed with ear canal cholesteatoma n I was wondering if there is any alternative other than surgery to cure the problem? And what can cause the problem to get worse?
Hi there, since the author of this post is still a medical student, we will redirect your question to our resident ENT surgeon. Thank you.
Thanks for the note, Hidayah/ Chief Editor.
Hi Elieza,
Surgery is warranted if the disease cannot be cleared be outpatient clinic procedure of suctioning & clearing the debris. Usually it is painful when deep. We advocate frequent follow up, softening of wax & ear toilet if disease is not extensive.
Infection can worsen the progress. Of course the spread to deeper structures of ear canal / temporal bone will favour for surgery to prevent it from invading vital structures such as facial nerve and the brain.