Perhaps you have read my previous article on swollen lymph glands in the MMG (https://www.mmgazette.com/should-i-be-worried-if-i-have-swollen-lymph-glands-dr-ahmad-nordin/). I did mention that the glands can become from a solid structure into a soft fluctuant swelling filled with pus.
I do caution to those of you eating at this moment. You may lose your appetite looking at few of the following images.
The condition will usually start with a small swelling with pain and subsequently with fever. There may also be associated toothache, throat pain, difficulty in swallowing, scalp infection or other head & neck symptoms- depending on the site of initial infection.
We notice here (Image 1), the left neck is swollen and red. We mark the skin on where the incision is supposed to be made.

Image 1: Neck abscess appearance before the surgery
We usually perform a Computed Tomography scan (CT scan) to assess the extension of the abscess and to exclude involvement of vital structures in the neck (Image 2). This is also due to the complicated multiple compartments which are interconnected in the neck.
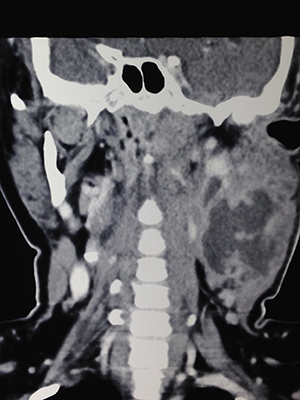
Image 2: Collection noted at the left neck (irregular black shadow at the centre of the swelling- at the right middle side of image)
The surgery is usually done under general anaesthesia. The area is cleaned with povidone iodine and draped (Image 3).
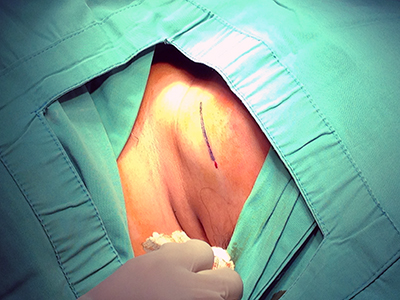
Image 3: Area cleaned and draped.
Initial incision is made with a blade on the skin (Image 4).
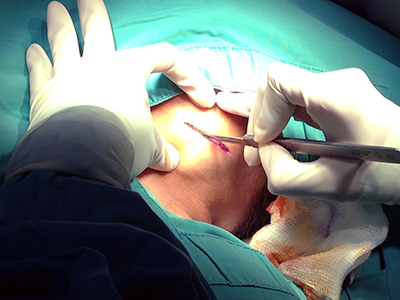
Image 4: Skin incision
Subsequent dissection is done with diathermy machine (Image 5). This reduces the effect of bleeding. I have mentioned the use of diathermy in my previously article about tonsil. (https://www.mmgazette.com/pembedahan-tonsil-bagaimanakah-caranya-dr-ahmad-nordin/)
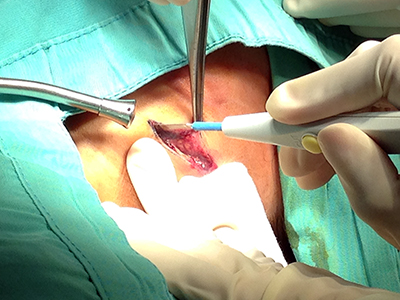
Image 5: Dissection with diathermy.
The skin edges are separated with retractors. Dissection is continued until the abscess capsule is identified. An initial small nick is made. Once the layer is breached, pus will start pouring out. A bacterial culture and sensitivity sample is taken with a sterile cotton swab and later to be placed in a special transport media (Image 6).
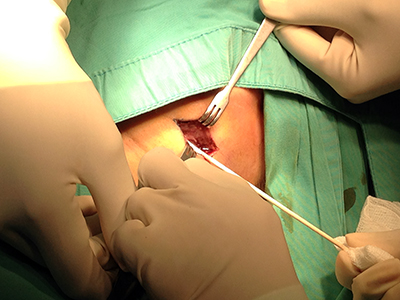
Image 6: Sample taken for bacterial culture & sensitivity.
The deep incision is then widened with blunt artery forceps to facilitate drainage of the rest of the thick pus (Image 7). In this patient, about 30ml of pus was evacuated.

Image 7: Thick pus flowing from the abscess.
The abscess usually has multiple compartments separated by thin membranes. These cavities need to be broken down to drain out the smaller pockets of pus. Using gloved finger is the safest option to avoid damage to surrounding vital structures (Image 8).
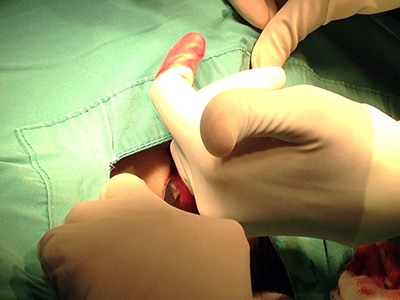
Image 8: Breaking the pockets of pus with a gloved little finger.
The cavity is cleansed with normal saline using a large syringe to clear the pus and blood (Image 9). This is done repeatedly until the return fluid is clear.
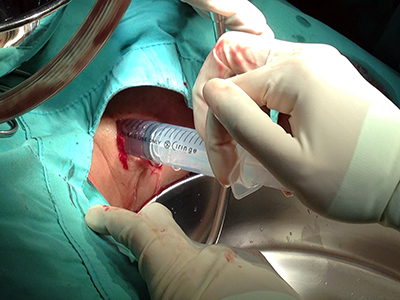
Image 9: Flushing of abscess cavity.
At the end, ribbon gauze is inserted into the cavity (Image 10). This is to prevent the cavity from collapsing. We prefer the cavity to be able to have an outlet for it to drain in the first few days. If it closes too early, pus will be trapped and the same problem recurs.
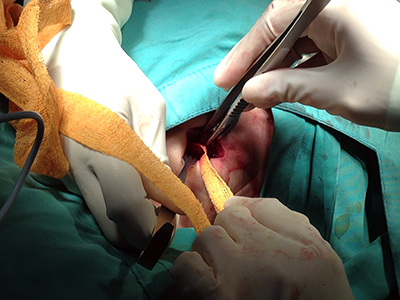
Image 10: Packing of abscess cavity with ribbon gauze.
Final step is to cover the wound with gauze and a pressure dressing (Image 11). Wound inspection is usually done the next day.

Image 11: Neck dressing applied at end of procedure.
Dressing is done daily. Once the wound is clean and fever subsides, the patient is allowed home. The patient needs to go for daily dressing in the clinic until his wound is clean. With good care, most of the wound will close without needing any suturing.
I hope I manage to educate and still keep your appetite at the same time for the minority of you readers of MMG!
(Acknowledgement: I once again would like to thank the patients, parents & staff for allowing their pictures to be published for public health education)
Dr Ahmad Nordin is an Ear Nose and Throat surgeon currently working in Sabah. Find out more about him on The Team page.
References:
- http://www.entslc.com/neck-abscesses accessed on 3 April 2014
- http://www.throatdisorder.com/surgeries/neck-abscess-incision-and-drainage accessed on 3 April 2014
[This article belongs to The Malaysian Medical Gazette. Any republication (online or offline) without written permission from The Malaysian Medical Gazette is prohibited.]